A Turning Point for Parental Choice, Medical Freedom, and Childhood Health Policy
On January 5, 2026, the CDC director signed a decision memorandum announcing a significant change to the routine childhood vaccine schedule. The COVID-19, influenza, hepatitis A and B, rotavirus, and meningococcal vaccines are no longer recommended routinely for healthy children. For the first time, parental choice and individual risk assessment are being placed ahead of one-size-fits-all mandates.
The CDC will continue to organize the childhood immunization schedule into three categories:
- Immunizations Recommended for All Children
- Immunizations Recommended for Certain High-Risk Groups or Populations
- Immunizations Based on Shared Clinical Decision-Making
The first category includes vaccines for measles, mumps, rubella, polio, pertussis, tetanus, diphtheria, Haemophilus influenzae type B (Hib), pneumococcal disease, human papillomavirus (HPV), and varicella (chickenpox). This represents fewer than 40 doses, compared to nearly 100 doses under the prior schedule when annual COVID-19 and influenza shots are included.
My lawsuit against the CDC, Thomas v. Monarez, was filed by attorney Richard Jaffe on behalf of Dr. Paul Thomas, Dr. Kenneth Stoller, and Stand for Health Freedom in federal court in Washington, D.C., in August 2025. The action remains open, and it is our hope that it may ultimately result in all routine childhood vaccinations being removed from Category 1 and placed into Category 3—shared clinical decision-making.
A second hoped-for outcome is that companies and individuals involved in administering vaccines will once again have liability for harm caused by vaccines once those products are no longer on the routine childhood schedule. This would effectively place vaccines back in line with other pharmaceutical products and medical interventions.
The removal of mandates and the restoration of liability for harm are essential steps toward restoring parental authority over what happens to their children. No doctor, politician, government agency, or public health authority should have the power to mandate medical treatments for healthy individuals. The COVID era revealed how corrupted and incapable of common sense and proper scientific analysis many institutions were—and, in many cases, still are.
We are not free from the tyranny of mandated childhood vaccination schedules until every parent has the right to informed consent and the unquestioned right to say no thank you to any medical procedure. It is time to end one-size-fits-all medicine and return to individualized care that respects natural immunity, personal choice, and diverse lifestyles.
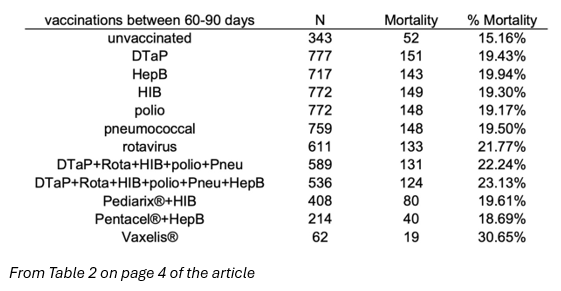
We are about to expose the biggest lie in medicine. As more parents opt out of the vaccine paradigm, the growing population of unvaccinated children will provide real-world data. That data will continue to confirm what my research and multiple independent datasets have already shown: unvaccinated children are significantly healthier than their vaccinated peers.
Imagine a world where rates of autism, ADHD, asthma, infections, chronic illness, allergies, and autoimmune disease are reduced by 50 to 90 percent. That future is entirely possible—and likely—once mandates and coercion end and parents are free to follow the science conducted by researchers who are not beholden to pharmaceutical or political pressure.
Dr. Paul (retired)
Just A Mom Notes:
For those of us parents who have children injured by vaccines, this feels like a breath of fresh air. A schedule that mandates any vaccine simply doesn’t make sense to me. Informed consent is critical. If you don’t know what you’re putting into your child’s body, how can you know whether you’re truly okay with it?
Blind trust doesn’t work anymore. COVID taught us that. The countless childhood illnesses and injuries linked to vaccines have taught us that as well.
I also struggle with the fact that if a product causes harm to me or my child, and I can’t hold anyone accountable because I was told it was “safe,” that responsibility somehow disappears. The idea that a doctor can dismiss a family from their practice because a parent chooses not to vaccinate their child is unacceptable to me. Why? Because they don’t go home with us afterward to care for our children. They don’t pay for the therapies, services, or lifelong support required when a child is harmed. They don’t live with the consequences—families do.
I know that for those of us who are relying on Kennedy to help make these changes, the process can feel slow. Please understand the pressure he is under. He is going up against a Goliath.
I urge parents to stand up for their children. My niece, whom I love dearly, has shared that she plans to vaccinate only what is required for school. Many people feel the same way. There are only five states that do not allow exemptions. In my opinion, exemptions exist because vaccines have not been tested against true placebos.
We are supposed to be living in the land of the free, yet mandates do not reflect that principle. My request has always been the same: become as informed as you possibly can. Make decisions based on your own health history and your family’s history. Remember—God gave us an immune system. Let’s use it.
— Just a Mom
— Just a Mom
#KidsFirst4Ever, #ParentalChoice, #InformedConsent, #MedicalFreedom, #PediatricHealth, #VaccinePolicy, #SharedDecisionMaking, #HealthFreedom, #FamilyHealth